Gastrointestinal and Hepato-pancreatico-biliary cancers- all you need to know?
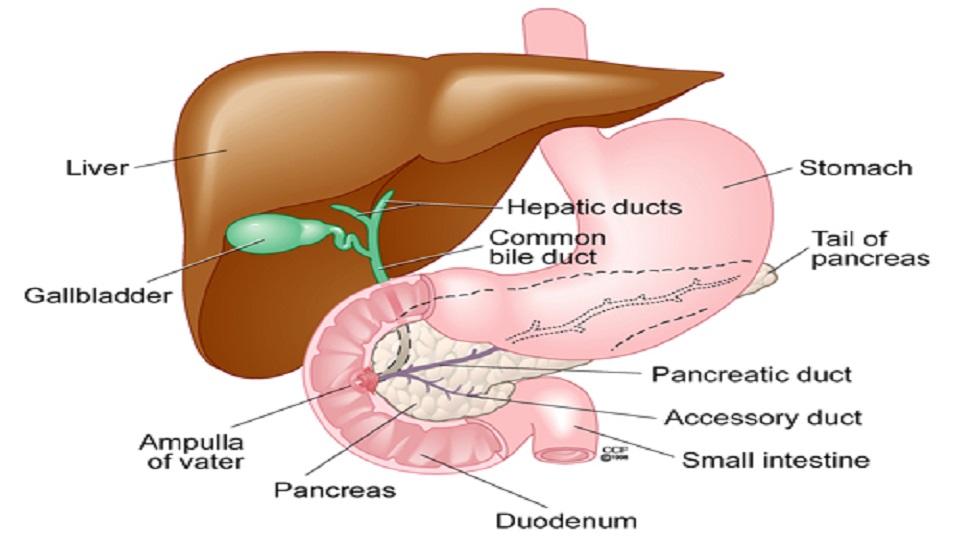
Gastrointestinal and hepato-pancreatico-biliary cancers include the cancers of the gastrointestinal tract like esophagus, stomach, duodenum, small bowel, colon and rectum. The hepato-pancreatico-biliary cancers include the cancers of the liver, bile duct, gallbladder and pancreas.
This article will highlight the presentation, early detection, diagnostic and staging modalities and treatment options for these cancers in general and also explain why you need to visit a specialist for these cancers.
How do these cancers present?
Most of these cancers in our country are detected at an advanced stage i.e. stage 3 and 4. Stage 3 implies that the spread is loco-regional, for example, to the nearby lymph nodes or adjacent organs, whereas in stage 4 disease the cancer spreads to the distant organs, for example stomach cancer spreading to the liver, lungs, peritoneum or distant lymph nodes. The symptoms vary depending on the organ involved by the cancer, the extent of involvement of the organ, for example an early stage cancer of stomach would present with minimal symptoms, whereas an advanced cancer usually present with pain, vomiting, weight loss and decreased appetite.
Is an early detection of these cancers possible?
Detection of these cancers at an early stage can result in an improvement in cure rates. There needs to be a lot of emphasis on awareness regarding the red-flag or warning symptoms amongst the public as well as general healthcare practitioners, who are the first point of contact in most parts of our country. This can help the patients to seek timely consultation and the general practitioner to refer the patient to the concerned specialist at the earliest. Similarly, screening programs are helpful in early detection. The main limitation of these programs is their cost-effectiveness, and hence their implementation in a vast country like ours is challenging. However, screening programs can be selectively implemented using simple screening methods in regions with a high incidence of a particular type of cancer specific to that region.
How are these cancers diagnosed?
The modality chosen for the diagnosis of gastrointestinal cancers depends on the site involved by the cancer. For example, diagnosis of cancers involving esophagus, stomach, duodenum, colon and rectum is done using endoscopy and biopsy from the growth. Ultrasound of abdomen done by an experienced radiologist is the initial investigation, which can detect or suspect cancers of the gallbladder, liver, pancreas and bile duct etc.
How are these cancers staged?
Cancer staging done before starting the treatment is also called clinical staging. This is essential to formulating the treatment plan and helps in prognostication. Commonly used staging investigations include CT scan, MRI, PET scan, etc. However, the staging investigations are determined by the tumor site and type. For example, staging investigations for a stomach adenocarcinoma include a CT scan of chest, abdomen and pelvis. However, a Ga-DOTANOC PET scan is essential to stage a neuroendocrine tumor of stomach.
Is tissue diagnosis or biopsy required in all cases?
A tissue diagnosis should be obtained whenever it is possible in the form of biopsy, cytology or cell block.
Tissue diagnosis is important
- Before start of cancer directed therapy like chemotherapy and/or radiotherapy
- To know the type of tumor, because the treatment varies with the cancer type i.e. to differentiate between a lymphoma, adenocarcinoma or other tumors
- When biopsy can alter plan and intent of management e.g: obtaining a tissue from a suspicious liver lesion in carcinoma stomach
- To differentiate some cancerous conditions from conditions which mimic cancer like tuberculosis, sarcoidosis etc
Tissue diagnosis is not however mandatory in some situations. These include When a negative biopsy will not alter the plan, for example, a radiologically convincing pancreatic or gall-bladder mass that is resectable on imaging and patient is fit for surgery.
Introducing a biopsy needle in such a situation also has a potential for tumor spread (approximately 1%) along the needle tract.
How are these cancers treated?
The treatment of these cancers depends on the clinical stage, tumor type, patient’s overall performance status, associated medical problems and patient preference. In general, in most of the early stage (stage I) cancers surgery is the treatment of choice. For most of the higher stage cancers with limited spread (stage II,III), a combined treatment with different modalities like chemotherapy, radiotherapy and surgery ensures better outcomes compared to a single modality approach. The intent of treatment is mainly palliative in majority of the stage IV cancers. However, there are stage IV cancers for example selective cases of colorectal, neuroendocrine cancers where multimodality treatment followed by surgery can result in cure.
Whom to consult for treatment of gastrointestinal cancers?
The management of these cancers is complex. Treatment is best delivered by a team of clinicians who are exclusively trained and experienced in their respective fields. In today’s day and age, oncology is moving towards organ-based specialization and practice and this has been shown to improve clinical outcomes.
It is therefore preferable to consult clinicians with exclusive training and expertise in managing gastrointestinal cancers.
Dr Abhishek Mitra
MBBS, MS, DNB Gastrointestinal Surgery (Sir Ganga Ram Hospital), HBNI Fellowship GI and HPB Oncology (Tata Memorial Hospital, Mumbai)
Senior Consultant,
Dept of GI and HPB Surgery, GI and HPB Oncosurgery, Minimal Access Surgery
Dharamshila Narayana Superspeciality Hospital, New Delhi
W Pratiksha Hospital, Gurugram
Apollo Spectra, Gurugram
Kalyani Hospital, Gurugram